How Psychological Evaluations Affect Injury Claims
Written By: Michael Vale, Content Writer
Medically Reviewed By: Dr. Cathy Colet, Psy.D., Licensed Psychologist
Last Reviewed: June 7, 2026
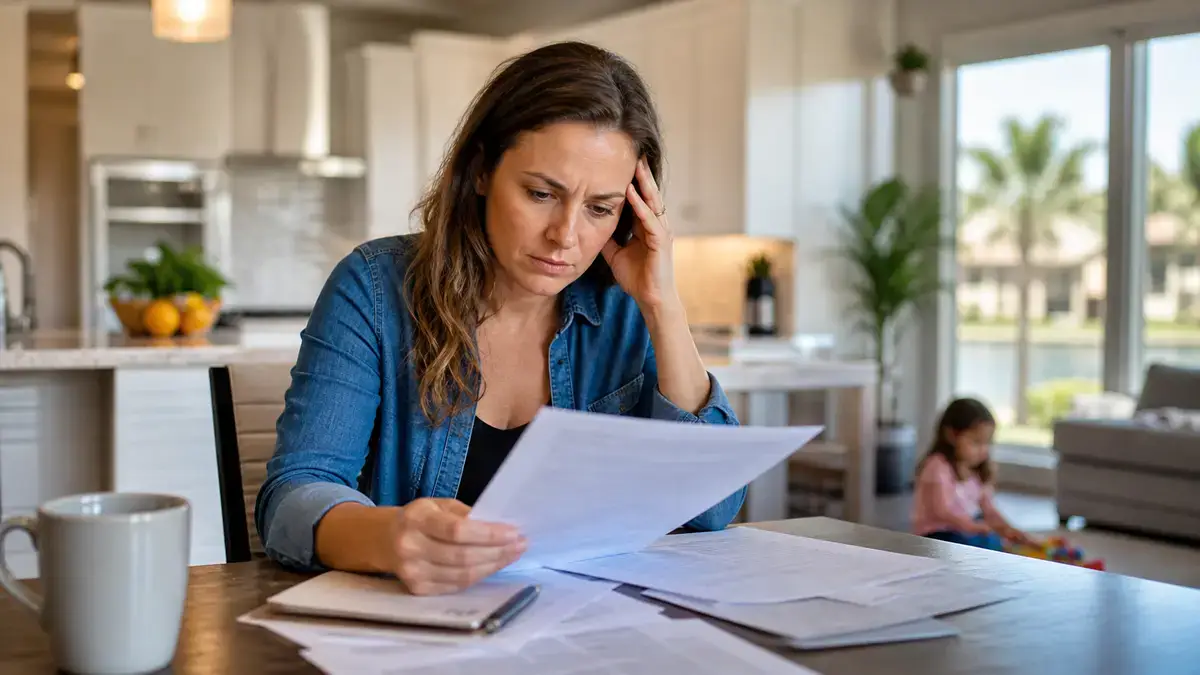
If you were hurt in an accident and you’re still not sleeping, still flinching at car horns, still not yourself, a personal injury psychological evaluation is how that damage gets put on the record. It’s an exam by a licensed psychologist that measures the mental and emotional harm tied to your injury, in language courts and insurers take seriously.
Most people think these cases are about broken bones and medical bills. They’re not, or not only. The part that’s hardest to prove is the part you can’t see.
A personal injury psychological evaluation is a structured assessment by a qualified psychologist that documents conditions like PTSD, depression, and anxiety caused by an accident or injury. It combines interviews, standardized tests, and a review of your records to link the harm to the event and explain how it affects your daily life.
We’ll cover what the exam includes, who runs it, what the tests can and can’t catch, and the one mistake that quietly sinks more claims than any other. We won’t talk about fees, and this isn’t legal advice.

What Does a Psychological Evaluation Do in a Personal Injury Case?
It turns invisible harm into evidence. That’s the whole job.
A car wreck leaves a dent the adjuster can photograph. Trauma doesn’t. So the evaluation does three things: it names the condition, ties it to the crash and not to something else, and shows how the symptoms hit your work, sleep, relationships, and daily function.
That third piece matters most, and a diagnosis alone is weak. “This person has anxiety” means little. “This person stopped driving, lost their job, and can’t be alone since the collision” is what moves a number.
What Is a Personal Injury Psychological Evaluation?
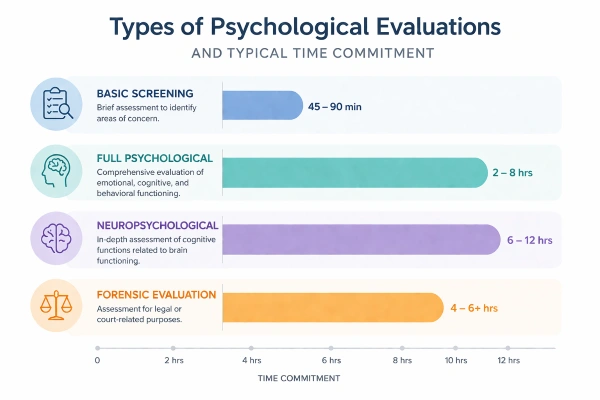
A personal injury psychological evaluation is a forensic mental health exam built for the courtroom, not the therapy room. A licensed psychologist runs it, usually over several sessions, and writes a report that can hold up if a lawyer tries to pick it apart.
That last part is the difference between this and regular therapy. Your therapist’s job is to help you feel better. A forensic evaluator’s job is to answer one question: what’s really going on, and is the injury the cause? Those are different jobs, and courts know it. A good evaluator stays neutral even when you’re the one who hired them.
How the Evaluation Process Works, Step by Step
Most evaluations follow the same path. It usually runs in this order:
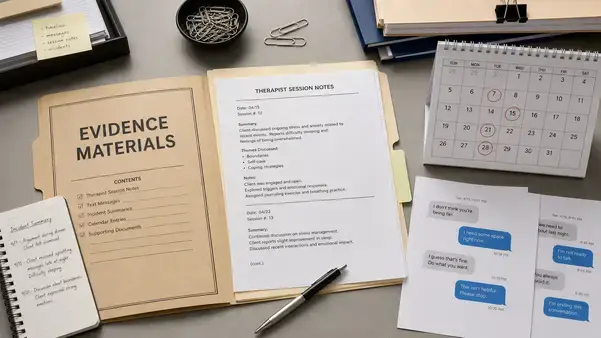
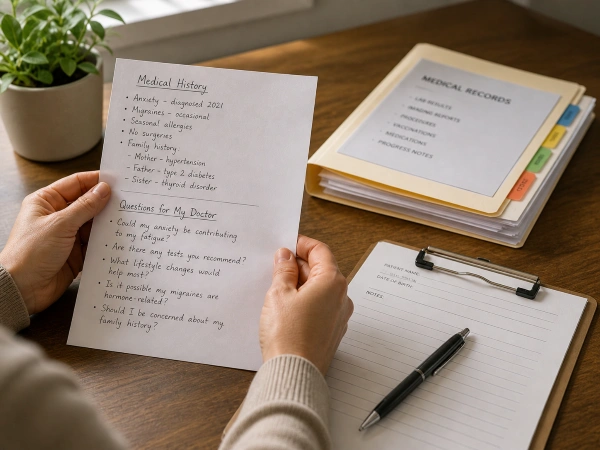
- Records review, covering your medical files, accident reports, and prior mental health history
- A clinical interview, often spread across two or more sessions
- Standardized testing
- Collateral interviews with people who know you
- A written report, usually 10 to 20 pages
Expect several weeks total. A little preparation goes a long way, so it helps to know how to prepare for the assessment before your first session. The four parts below are where the real work happens.
Records Review and the First Meeting
Before you say a word, the psychologist reads your file. That’s deliberate. They want your history, including any anxiety or depression that predates the accident, so the defense can’t ambush them with it later. The first meeting sets the frame. Who they are, who they’re not, and the fact that this exam isn’t a treatment.
Which Tests Get Used, and Why
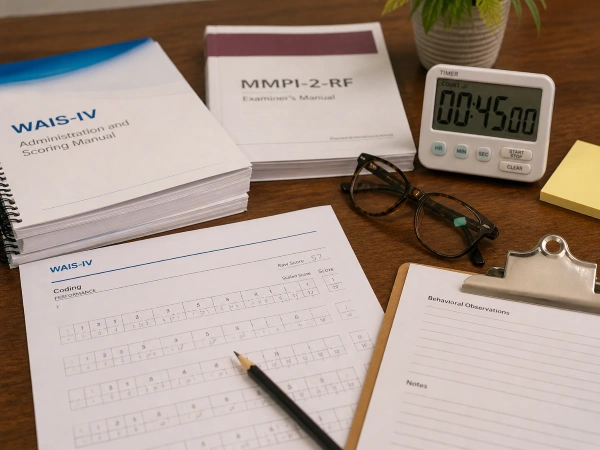
In plain language, the tests measure your symptoms and check whether you’re being straight. Common ones include the MMPI-3 and the PAI, both packed with validity scales that flag exaggeration or faking. For suspected memory or attention problems, evaluators add symptom-validity measures like the TOMM. No single score decides anything. A skilled evaluator reads the whole picture, not one number. If a head injury is in play, the work may extend into neuropsychological testing.

The Clinical Interview
This is a long conversation, often hours across more than one session. The evaluator asks about the accident, your symptoms, your sleep, your work, and your life before all of it. They’re also watching how you tell it and whether your account stays consistent. Consistency is everything. People who try to sound worse than they are get caught, and people who downplay real symptoms hurt their own case.
Talking to People Who Know You
With your permission, the evaluator may call your spouse, a close friend, or your regular doctor. Not to snoop. To corroborate. If your partner describes the same nightmares and short temper you reported, your account gets stronger. If nobody else has noticed any change, that’s a problem the report has to address.

Common Conditions These Evaluations Uncover
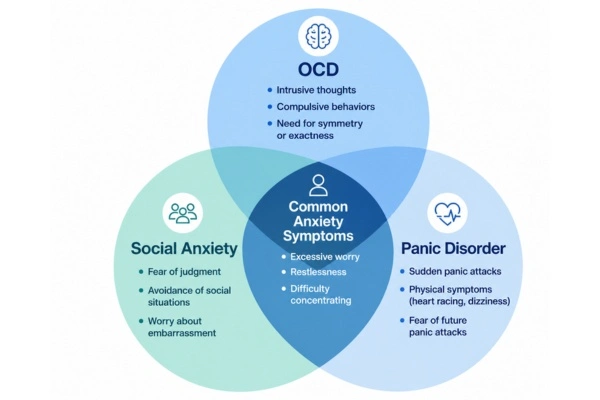
Three conditions show up again and again after a serious injury: PTSD, depression, and anxiety.
PTSD is the big one in accident cases. Flashbacks, nightmares, panic at anything that reminds you of the crash, avoiding the road where it happened. Depression often follows when the injury steals the life you had, your job, your sport, your independence. Anxiety can attach to the injury itself or to the slow grind of the legal process.
There’s overlap with the body, too. Chronic pain feeds depression. A head injury from the same collision can blur the line between emotional symptoms and cognitive ones, which is exactly when a careful evaluation earns its keep.
How Evaluations Shape Case Outcomes in 2026
A solid evaluation can move a case in either direction, which is the part people forget.
Link serious harm to the injury, and the value of the claim goes up, because the law treats emotional damage as real damage. Find little harm, or harm from another cause, and it can shrink the claim or sink it. Both sides use these exams. Yours strengthens your case. The other side is hired to test it.
Do These Evaluations Affect Settlement Value?
Yes, sometimes a lot. Documented psychological injury feeds the non-economic part of a claim, the pain-and-suffering side that often dwarfs the medical bills. One 2025 review of more than 5,800 personal injury cases put the average settlement around $55,000, with the high end driven by severe, well-documented harm. No evaluation guarantees a bigger check, and anyone who promises one is selling something. It gives your damages a factual spine instead of a feeling.

Expert Testimony and the Battle of the Experts
If the case goes far enough, your evaluator may testify, explaining the diagnosis, cause, and impact in plain terms a jury can follow. When both sides bring an expert, you get a battle of the experts. It rarely cancels out. The winner usually has stronger credentials, cleaner methods, and findings that fit the evidence. Board certification helps, and so does an evaluator who has survived cross-examination.
Is a Personal Injury Psychological Evaluation Confidential?
Short answer: no, not the way therapy is. This surprises people, so read it twice.
Treatment is protected. A forensic evaluation is the opposite. It exists to be shared with the attorneys, the court, and the other side. The psychologist’s loyalty isn’t to your comfort. It’s to an honest answer, the kind professional ethics rules require no matter who’s paying. A good evaluator tells you this up front, so nothing you say feels like a trap later. Anyone who frames a litigation exam as private like a counseling session is a red flag.
Where Psychological Evaluations Fall Short
These exams aren’t perfect, and pretending otherwise helps no one.
Psychological injury is subjective. There’s no X-ray for trauma. That opens two real risks. One is malingering, the clinical word for faking or padding symptoms, which gets tempting when money is on the line. Good tests catch a lot of it, not all. The other risk runs the other way. A thin, sloppy report can get thrown out under the reliability standard judges apply to expert testimony, sometimes called the Daubert standard.
Why a Truly Neutral Evaluator Matters
Because the whole report is only as good as the evaluator’s independence. A one-sided exam is worthless the moment it’s challenged.
The industry loves the phrase “neutral and unbiased.” The uncomfortable truth is that complete objectivity is a goal, not a finished state. Even careful, ethical evaluators carry blind spots, a point forensic specialists make in their own peer-reviewed research. The guidelines that govern the field, recently extended through the end of 2026, ask evaluators to aim for fairness, weigh rival explanations, and stay independent precisely because bias is the default, not the exception.
So what protects you? Method. A neutral evaluator runs the same tests, asks the same hard questions, and follows the same logic no matter who signed the check, which is the standard we hold ourselves to at our forensic psychology practice. It’s also why a one-sided hired gun gets shredded on cross, and why an evaluator who works both plaintiff and defense cases carries more weight with a jury.
So, Is It Worth Getting One?
If your injury came with real psychological harm, the kind you can’t see but live with every day, then yes. Documenting it is how it counts.
Skip it and the most painful part of your injury stays invisible to the people deciding your case. The one mistake I’d warn against is waiting too long, or using someone without forensic training to save a step. A weak evaluation is worse than none, because the other side will use it against you.
Get the right evaluator early, be honest, and let the work speak. A well-run personal injury psychological evaluation won’t promise you an outcome, but it will make sure the harm you carry is on the record, in language the system respects. The strongest practices also stay visible online, so the attorneys and clients who need that work can find it.
FAQs
What is a personal injury psychological evaluation?
It’s a forensic mental health exam that documents psychological harm, such as PTSD or depression, caused by an accident or injury. A licensed psychologist runs it over several sessions and writes a report built to hold up in court. Unlike therapy, its purpose is to answer a legal question, not to provide treatment.
How long does a personal injury psychological evaluation take?
Most take several weeks from start to finish. The interviews alone can run several hours across two or more sessions, and the psychologist still needs time for testing, records review, and a report that often runs 10 to 20 pages. Complex cases with heavy records take longer.
Is a forensic psychological evaluation confidential?
No, not the way therapy is. A forensic evaluation exists to be shared with the attorneys, the court, and the opposing side. A good evaluator explains this before you start, so nothing you say is mistaken for a private counseling session.
What tests detect faking or exaggerated symptoms?
Forensic psychologists use instruments like the MMPI-3 and the PAI, which include built-in validity scales that flag inconsistent or exaggerated reporting. For memory or attention complaints, they add symptom-validity tests such as the TOMM. No single score is decisive; the evaluator weighs the whole pattern against your records and interview.
Can the defense make me see their own psychologist?
Often, yes. The defense can request an independent medical examination, or IME, with a psychologist of their choosing. That sets up a battle of the experts, where the more credible, better-documented opinion usually carries the most weight.
Is a letter from my treating therapist enough?
Usually not for a contested claim. Treating therapists are valuable, but courts often discount their letters because of the therapeutic alliance and the lack of forensic testing. An independent evaluation built around objective measures and the Daubert reliability standard holds up far better under cross-examination.

Dr. Cathy Colet, Psy.D., is a Licensed Clinical and Forensic Psychologist and founder of FC PsychExperts in Jupiter, Florida. She provides expert witness testimony across criminal, family, and immigration law, with advanced training in competency evaluations, criminal responsibility, child custody assessments, and VAWA hardship waivers.