What To Do When A Child Refuses Reunification Therapy
Written By: Michael Vale, Content Writer
Medically Reviewed By: Dr. Cathy Colet, Psy.D., Licensed Psychologist
Last Reviewed: June 16, 2026
Start with this. If your child is refusing reunification therapy, forcing it is the fastest way to make things worse. A 2024 study of adults who did intensive reunification programs as kids found worse relationships with the targeted parent later, not better. Pushing harder hardens the bond.
Reunification therapy is a structured family treatment meant to rebuild trust between a child and a parent they’ve grown distant from, usually after a divorce or custody fight. A trained clinician works with both sides, over several months, at the child’s pace.
This is about what to do when the child says no, not how to win a contempt motion.

Why Do Kids Refuse Reunification Therapy?
Kids refuse for three reasons. Loyalty to the parent they live with, real fear, or dread of the unknown. Which one you’re facing drives your next move.
The field still can’t agree on what reunification therapy even means. A March 2024 Association of Family and Conciliation Courts keynote said as much. So a child resisting a multi-day program that splits them from the parent they trust may have a point.
Responding When a Child Won’t Go
No single script works. The providers worth hiring go slow and never coerce. Compare the main options first.
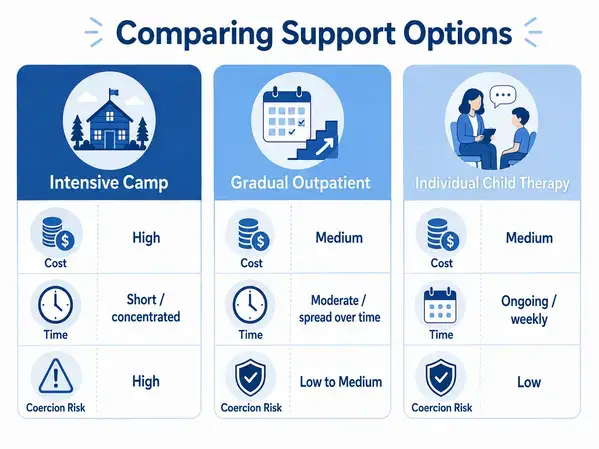
| Option | Typical cost | Time | Coercion risk | Best fit |
| Intensive residential program | $15,000–$40,000 / 4 days | Days, plus follow-up | High | Rarely; severe court-ordered cases, and contested |
| Gradual outpatient reunification | $175–$200/hr; ~$2,500 retainer | Ongoing, billed hourly | Low | Most families with a resistant child |
| Individual child therapy + co-parenting | Similar per session, fewer joint visits | Variable, often ongoing | Lowest | When safety or trauma comes first |
Outpatient reunification work is private pay, usually $175–$200 an hour, billed against a retainer starting around $2,500. Intensive camps cost far more. ProPublica reported a four-day program at $15,000, and others reach $40,000 or higher. Insurance rarely covers any of it. The priciest option is the riskiest one I’ve seen. A June 2025 Texas law curbed the most coercive programs, with other states following.
Start With an Honest Conversation
Before any therapy, talk to your kid. Not a pitch. A real talk where they name the fear and you don’t argue them out of it. Kids who feel heard show up less defended.
Ease In With Short Sessions
A good clinician starts small: a 20-minute meeting with the child and therapist alone, no estranged parent in the room yet. Trust builds in inches.
Does Play Therapy Help Resistant Kids?
For younger kids, often yes. Play lets a child show what they can’t yet say. Hand a guarded seven-year-old a sandtray and the walls drop. Forcing play on a teenager reads as condescending, so match the tool to the age, which good family therapy does anyway.
Take the Child’s Fears Seriously
A kid who says they don’t feel safe isn’t an obstacle. They’re a witness. If a child raises anything like fear of harm, screen for it before pushing reunification, not after. The American Psychological Association puts abuse screening ahead of any alienation theory. A January 2026 Family Court Review piece called the mess of vague court orders a near-lawless space.
The Custodial Parent’s Role
The parent the child lives with can make or break this. Treat therapy as punishment and the child reads it instantly. Send the same calm message as the other parent and the child settles. Agree on one thing: the child comes first, the standard behind high-conflict custody cases.

What Does Realistic Progress Look Like?
Slow, slower than you want. Progress isn’t a sudden hug, it’s a session that ends without tears. Actually, that’s not quite right. Progress is the child feeling less afraid, whether or not the bond looks repaired. Chasing a tidy reunion by a court deadline is how good cases go sideways.
What Makes a Good Reunification Therapist?
The right therapist is trained for court work, screens for safety first, and will tell you no when no is the honest answer.
Ask three things before you hire. What method do you use, and what evidence backs it? How do you handle it if my child says they were hurt? What happens if they refuse mid-process? A clinician promising a guaranteed reunion is selling something.
Credentials matter too. Look for training in court-involved therapy and family violence, not a generic counseling license. A practice handling court-ordered therapy and custody work knows the reports a judge needs.
Putting Your Child First
Hold onto one thing. Your child’s refusal is information, not defiance. It tells you what they’re scared of, exactly what reunification therapy must address before it works. Good outcomes come from slowing down, screening for real problems, and hiring an honest clinician, not from pushing hardest. If your child refuses reunification therapy right now, talk to experienced forensic psychologists who do this work locally and will tell you the truth.
FAQs
What happens if my child refuses to go to reunification therapy?
Courts usually expect the requesting parent to make a good-faith effort to encourage attendance. Persistent refusal can lead to findings of contempt, fines, or changes to custody, though judges weigh an older teen’s wishes more heavily. The stronger move is preparing the child, choosing a non-coercive therapist, and addressing the fear behind the refusal.
Does reunification therapy actually work?
The evidence is mixed and hotly debated. A 2024 study found adults who went through intensive programs as children reported worse long-term relationships with the targeted parent, while gradual, voluntary work tends to show better results. There is no professional consensus on what counts as success.
Can a court force my child into reunification therapy?
In most states, judges have wide discretion to order therapy in custody cases, even over a child’s objection. That is changing in places like Texas, where a 2025 law limits coercive programs and no-contact orders. Objections grounded in documented safety concerns carry more weight than general reluctance.
Is reunification therapy ever harmful?
It can be, especially the intensive, coerced versions. Documented risks include heightened distress, damaged long-term relationships, and retraumatization when abuse allegations are present. This is why the American Psychological Association and family court experts insist on screening for safety before any reunification work begins.
How do I find a good reunification therapist?
Look for training in court-involved work and family violence, not just a standard counseling license, and ask what evidence supports their method. A clinician who guarantees a fixed timeline or a happy reunion is a red flag. Membership in groups like the Association of Family and Conciliation Courts is a good sign.